Stimulating Muscles to Accelerate Rehabilitation
This year’s Stepping Strong Innovator Awards finalists are addressing complex challenges related to trauma research. Each of the three finalists hopes to receive the $100,000 Stepping Strong Innovator Awards, which will be announced online on Monday, Oct. 17. Read about their work below, and vote for your choice.

Giorgio Giatsidis, MD
Stimulating Muscles to Accelerate Rehabilitation – Giorgio Giatsidis, MD
What challenge does your project address?
Injuries to the legs and arms often destroy muscle, reducing both mass and strength. Today, there are almost no approved therapies or strategies—for use in conjunction with standard physical therapy—to induce muscle regeneration or accelerate recovery following trauma. Unfortunately, current interventions remain rudimentary, and prolonged hospitalization incurs further tissue damage.
Once home, trauma patients face a steep path of rehabilitation. I call this “the trauma iceberg.” That is, what we see—and treat—is only the tip of what our patients actually experience. This project aims to break the trauma iceberg by developing novel therapies to initiate muscle recovery immediately following the trauma, prevent the onset of further inactivity-induced damage and accelerate the rehabilitation path toward a normal life.
What is a compelling aspect of your project?
Our cells regenerate in response to mechanical stimulation. For example, when we go to the gym, we stimulate muscles by stretching and contracting them, and this activity makes them grow. These principles can also be used to design novel, safe, non-invasive and patient-friendly therapies.
This project seeks to address the burden of prolonged trauma rehabilitation by passively stimulating injured muscles to regenerate and accelerate their recovery directly at the bedside. To realize our goals, our team will determine the exact conditions to effectively promote mechanically induced regeneration of injured muscle and, in collaboration with engineers, integrate these findings into the development of a portable device that can be easily applied to trauma patients inside the hospital and at home.
How will your project benefit future patients who suffer from trauma-related injuries?
Traumatic muscle injuries to legs and arms are a very common and dramatic occurrence. Trauma care for these patients does not end with the treatment of acute, life-threatening conditions and wounds. It continues through the long, challenging path of rehabilitation.
Our proposed therapy and device will help to facilitate muscle regeneration in a hospital setting, prevent the onset of further damage and accelerate the path of rehabilitation.
CAST YOUR VOTE
or read more about the other Stepping Strong Innovator Awards finalists:
 21st Century Tools to Measure 21st Century Tools to Measurethe Progress of Bone Healing |
 Detecting Early Neurological Decline Detecting Early Neurological Declineto Prevent Paralysis |






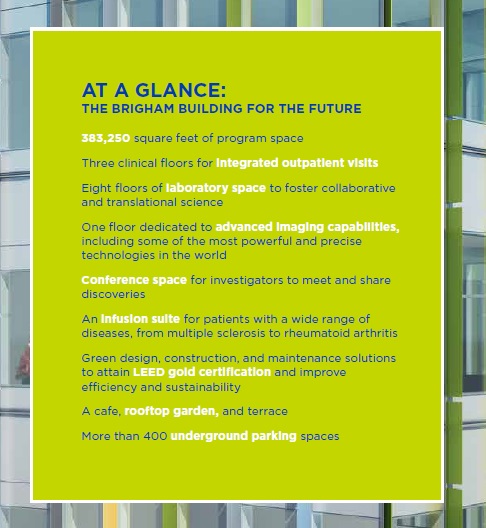
 BWHC’s Strategy in Action: Scalable Innovation
BWHC’s Strategy in Action: Scalable Innovation
 “I am most excited about the potential multidisciplinary collaborations that will occur on all levels—among basic scientists, clinical researchers and clinicians managing patients with state-of-the-art technology. Exposure and small interactions will hopefully lead to big discoveries.”
“I am most excited about the potential multidisciplinary collaborations that will occur on all levels—among basic scientists, clinical researchers and clinicians managing patients with state-of-the-art technology. Exposure and small interactions will hopefully lead to big discoveries.” “As a research RN who is about to move into the building, I am excited about the integration of research and clinical care under one roof. Both divisions depend on each other to accomplish the ultimate goal: health!”
“As a research RN who is about to move into the building, I am excited about the integration of research and clinical care under one roof. Both divisions depend on each other to accomplish the ultimate goal: health!” “It’s exciting to me because I’m working mostly in the building, and I love to be busy and interact with people.
“It’s exciting to me because I’m working mostly in the building, and I love to be busy and interact with people. “It is great that the researchers have space that is designed for collaboration. I am excited to be able to assist them with all of their audiovisual needs.”
“It is great that the researchers have space that is designed for collaboration. I am excited to be able to assist them with all of their audiovisual needs.” “The rooftop garden is such a great feature and really exciting, as is the new conference room space on the third floor. Overall, it’s exciting to have a new building open up, and it’ll be especially interesting to see the interactions between the research labs and clinics.”
“The rooftop garden is such a great feature and really exciting, as is the new conference room space on the third floor. Overall, it’s exciting to have a new building open up, and it’ll be especially interesting to see the interactions between the research labs and clinics.” “The new building will bring physicians of different disciplines together to work on some of our most challenging medical problems. Researchers will also be close by to apply the newest research techniques to develop innovative therapies.”
“The new building will bring physicians of different disciplines together to work on some of our most challenging medical problems. Researchers will also be close by to apply the newest research techniques to develop innovative therapies.” “It’s exciting to me to see a new ‘green’ research building that will allow us to expand into new areas and continue providing excellent patient care.”
“It’s exciting to me to see a new ‘green’ research building that will allow us to expand into new areas and continue providing excellent patient care.” “Our core values are healing and compassion, and I believe the new building will support this environment for our patients and families.”
“Our core values are healing and compassion, and I believe the new building will support this environment for our patients and families.” “I am excited for the grand opening of the new building. I am glad to see most of our researchers located back on the main campus. I look forward to supporting the many research efforts with behind-the-scenes tech support from our audiovisual team.”
“I am excited for the grand opening of the new building. I am glad to see most of our researchers located back on the main campus. I look forward to supporting the many research efforts with behind-the-scenes tech support from our audiovisual team.”

























 BWH and the Department of Neurology mourn the loss of H. Richard Tyler, MD, former chief of the Division of Neurology and BWH’s first full-time neurologist. He passed away May 9 at the age of 88.
BWH and the Department of Neurology mourn the loss of H. Richard Tyler, MD, former chief of the Division of Neurology and BWH’s first full-time neurologist. He passed away May 9 at the age of 88.