Q&A: Creating Pathways for the Next Generation of Diverse PAs
Audrey Fritzinger, MMSc, PA-C, joined the Brigham three years ago as a physician assistant (PA) in Interventional Radiology and now cares for patients in both Cross-Sectional Interventional Radiology as well as the Division of Angiography and Interventional Radiology. In addition to her clinical work, she leads several diversity, equity and inclusion (DE&I) activities for PA Services.
Fritzinger recently spoke with Brigham Bulletin about her work as a PA and her commitment to expand opportunities for more PAs of color.
What’s your career path been like so far?

Audrey Fritzinger
AF: I was introduced to the PA profession through federally qualified health centers (FQHCs) in Philadelphia. I always knew I wanted a career with an intersection of medicine and public health, seeing the PAs in practice helped me solidify the decision to pursue a career as a PA. As a student at Yale, I did a rotation in the ICU at Yale New Haven Hospital, learning to practice critical care medicine in an urban environment. This helped guide me toward a position in the ICU after graduation, I loved practicing critical care medicine and performing procedures, and I really enjoyed utilizing ultrasound as a means to perform bedside procedures and evaluate progression of critical illness. When my time in the ICU came to an end and family brought me to Boston, I found my calling in interventional radiology, a specialty which is the perfect intersection of critical care, procedural and outpatient medicine.
Let’s talk more about your involvement in DE&I. What inspired you to become engaged in this work?
AF: My involvement DE&I work started when I was in high school. I attended predominately white high school and college and was involved in many extracurricular activities in this realm. This continued as I transitioned to PA school at Yale.
Yale is a predominantly white institution, and the PA profession is occupied predominantly by white females. So, early on, I saw there weren’t a lot of providers, preceptors or faculty who resembled me. I had to look outside of the program for mentors.
I was lucky enough to work with Dr. Marcella Nunez-Smith and a group of medical students and nursing students to create an elective course called U.S. Health Justice. We felt that there were a lot of gaps in the curriculum in terms of things that were happening in New Haven and more broadly — things that we never discussed but saw in our rotations.
For example, we partnered with community organizations — including, but not limited to, the Needle Exchange Program and the Community Health Care Van — and we delved deep into other social determinants of health that we were not really discussing in medical lectures. The course is still ongoing, and it’s now been integrated into the curriculum.
It excited me to be involved in this great work, but in my post-graduate period of starting a new job in the ICU, other Yale students continued this work while my focus shifted for a brief period. I didn’t really do anything extracurricular just because of the crazy hours, so when I came to the Brigham, I realized that was something that I needed fulfilled.
What kinds of initiatives are you working on now?
AF: I read about a PA student at Morehouse College, Calbeth Alaribe, who participated in the MIT Healthcare Hackathon and whose group won an award. After an exciting conversation with her, bells went off that there might be an opportunity for the Brigham to partner with a historically black college and university (HBCU) and potentially positively influence the community here.
 I find it a privilege to be around Black people and to have that celebrated. Boston is not a historically diverse city. In a lot of spaces where I occupy, it’s not celebrated. I’m also not frequently around a lot of Black people, especially here at the Brigham. I wanted to see if we could diversify the PA workforce here at the Brigham.
I find it a privilege to be around Black people and to have that celebrated. Boston is not a historically diverse city. In a lot of spaces where I occupy, it’s not celebrated. I’m also not frequently around a lot of Black people, especially here at the Brigham. I wanted to see if we could diversify the PA workforce here at the Brigham.
Jess Logsdon [senior director of PA Services] and Rosann Ippolito [manager of PA Education] were very excited about this collaboration and how we can foster a relationship with an HBCU — potentially opening the doors for more PA students who might want to work here at Brigham.
The plan is to start with a cohort of students this spring to offer clinical didactics and mentorship, including one-to-one mentors of color aside from their preceptors.
Other training programs in medicine have a visiting period, whether it’s residency or fellowship, or they get paid opportunities to visit a program. As PAs, we don’t have that, so when you’re considering whether to take a job somewhere, you don’t get to have an extended visit at the institution beforehand. I think what we’re doing with this rotation is unique and will allow students to experience the culture firsthand and see how we practice medicine here at the Brigham.
What do you find most rewarding about this work?
AF: I’m not the only PA doing it. There are so many other PAs who are active in DE&I work at the Brigham. I had an idea, I asked for help and people came running to support it.
I get excited when others are just as enthusiastic about this work as I am — that this is as close to their heart as it is to mine. That makes me feel like I’m at the right institution and in the right community. It also makes me want to invite others to join, which is why I’m so excited and confident about opening the Brigham up to more PA students of color, because it’s a great place to be. I want them to be here and learn alongside us.
Physician Assistant Week is held annually Oct. 6–12 to honor physician assistants’ substantial role in improving health. In celebration of Brigham PAs and their involvement in nearly every facet of the care across the institution, Brigham Bulletin has highlighted one of the many exceptional physician assistants to cap off PA Week this year.










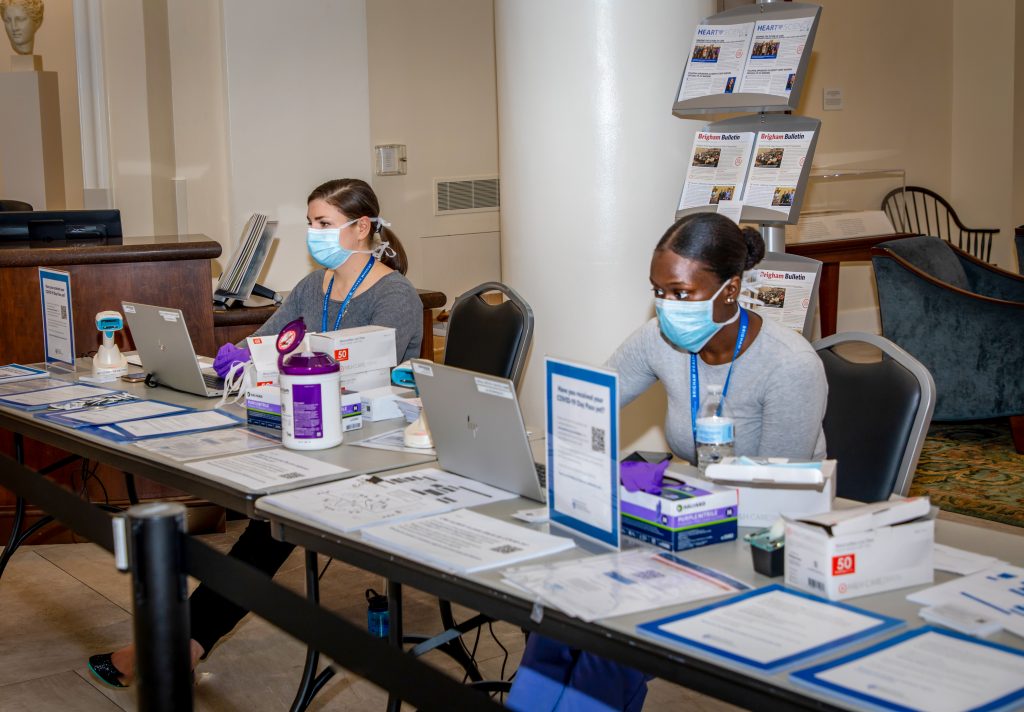
 Nurse Brieanna Gacek, RN, BSN, PCCN, helped open the first Special Pathogens Unit and Special Pathogens-Intensive Care Unit (ICU) during the first surge in spring 2020. Nearly one year later, she received a new assignment — to administer some of the first doses of the vaccine in the Hale clinic.
Nurse Brieanna Gacek, RN, BSN, PCCN, helped open the first Special Pathogens Unit and Special Pathogens-Intensive Care Unit (ICU) during the first surge in spring 2020. Nearly one year later, she received a new assignment — to administer some of the first doses of the vaccine in the Hale clinic.





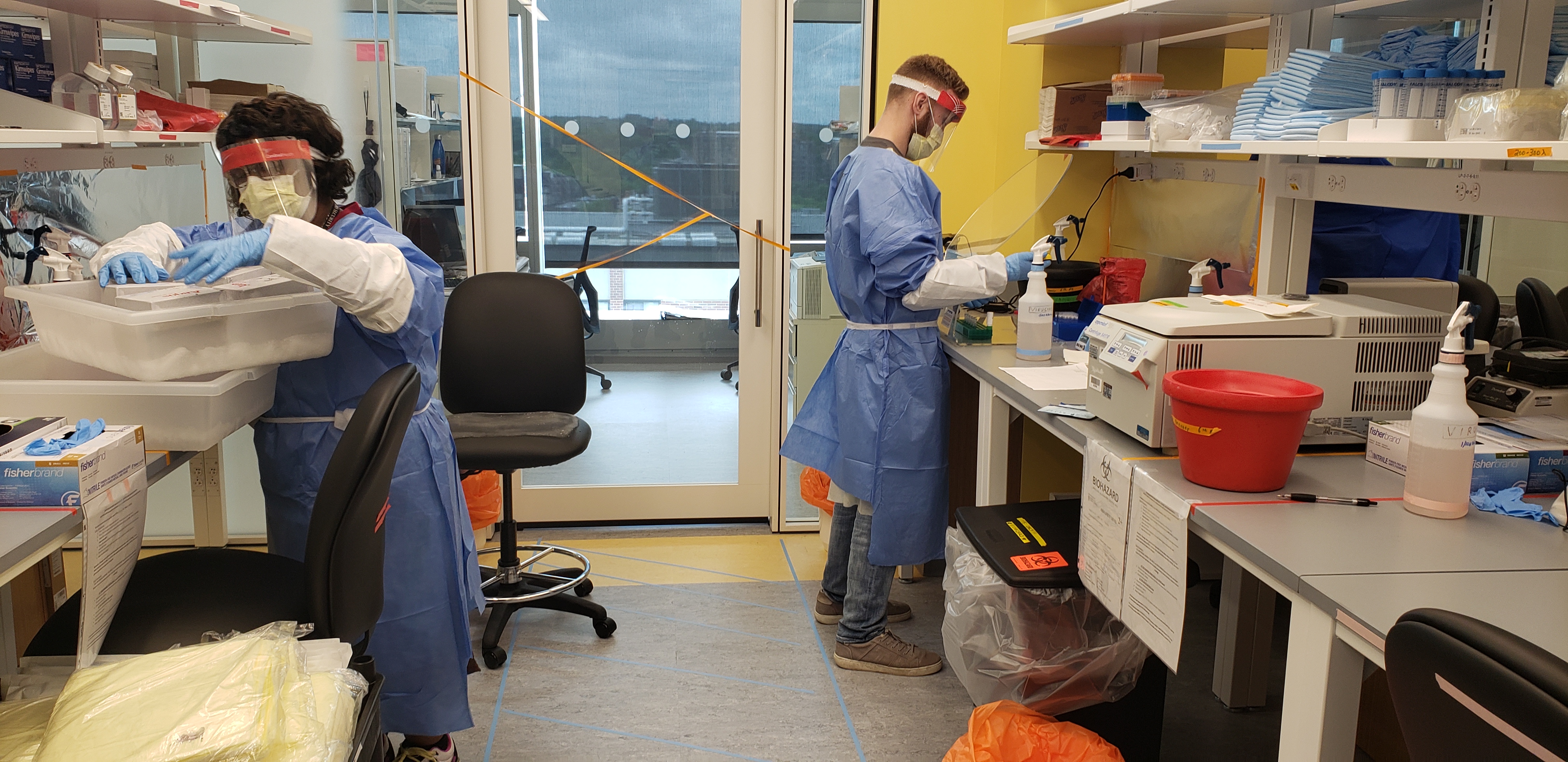
 “It needed to be multidisciplinary because everybody’s expertise was needed,” Dias said.
“It needed to be multidisciplinary because everybody’s expertise was needed,” Dias said.