BWHC Achieves Highest Flu Vaccination Rate to Date

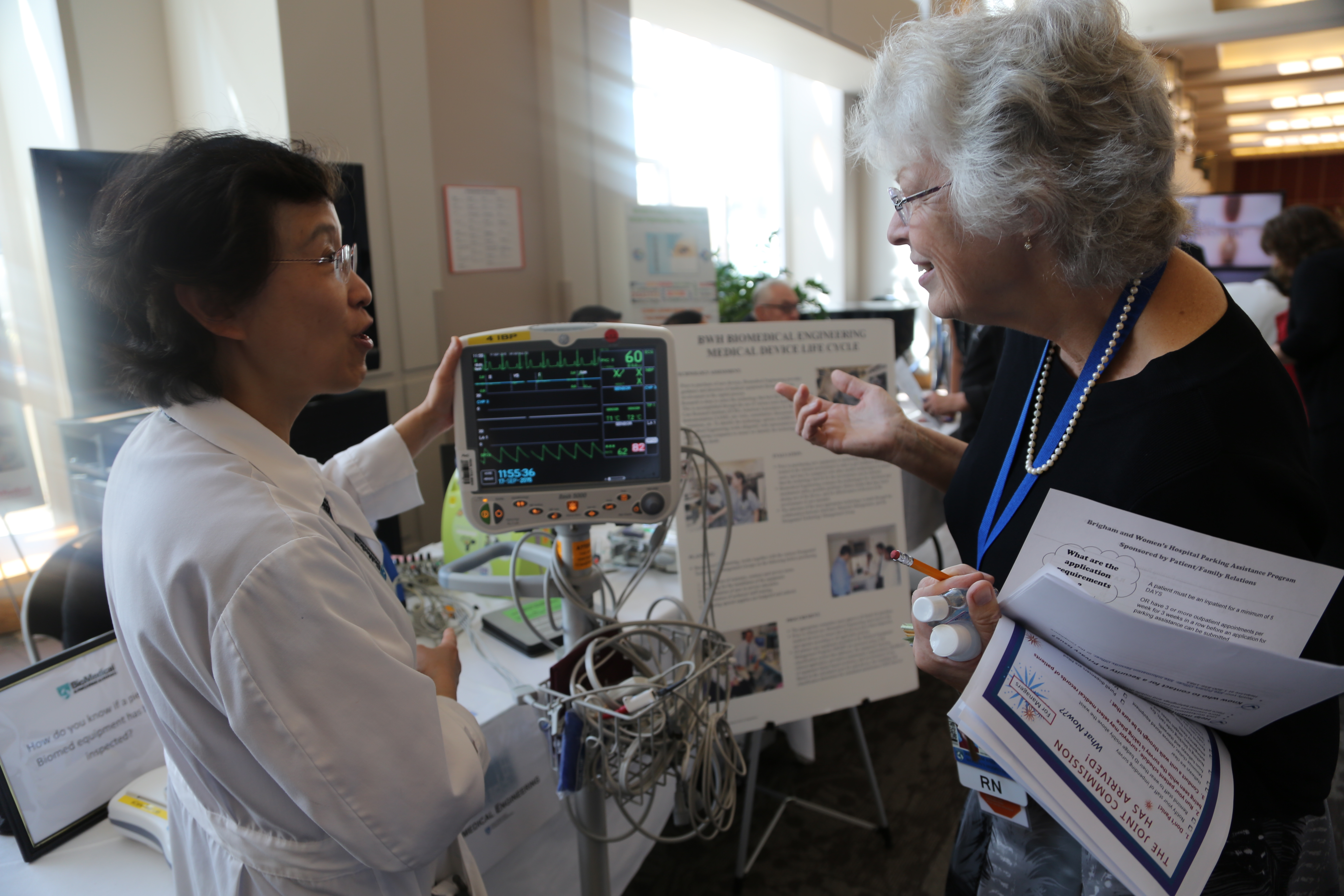
Susan Herman, a staff nurse in the Cardiac Cath Lab, receives her flu vaccine earlier this flu season.
With the implementation of a new flu policy at BWHC in 2015–2016, the employee vaccination rate has risen more than 12 percent from last season, with 89 percent of employees being vaccinated to date—the hospital’s highest employee vaccination rate ever recorded.
“Our flu vaccination rates are a testament to the remarkable commitment of our staff to the health and wellness of all who come through our doors,” said BWHC President Betsy Nabel, MD. “Thank you for all you do on behalf of our patients, their families and each other, not just during flu season, but always.”
Carin Bennett-Rizzo, MS, ANP-BC, COHN-S, director of BWH Occupational Health Services (OHS) and a member of the BWHC Flu Vaccination Task Force, credits managers and staff for helping to make this year’s hospital-wide flu vaccination program the most successful yet.
“BWHC had an extremely positive year related to increasing flu vaccination rates and decreasing the percentage of staff that declined the vaccine,” she said. “Our community worked together to better protect patients, families, staff and visitors from the spread of flu.”
For this flu season, BWHC made changes to its annual flu policy, requiring that BWH and BWFH personnel who are not vaccinated for influenza for any reason, including a medical reason, wear a surgical or procedural mask while they are in patient-care areas during flu season. In past years, despite education and improved vaccine access, overall employee vaccination rates were stuck at 75 to 80 percent.
The mask requirement is in addition to the Massachusetts state requirement that all employees must attest to either receiving flu vaccine or declining to be vaccinated. The end date for this flu season will be determined by BWH Infection Control based on state and local incidence of flu.
To date, 14,154 BWHC personnel have been vaccinated through OHS, the Peer-to-Peer program or their own provider; 1,610 people, or roughly 10 percent of employees, have declined vaccination. Last year, about 12,000 people were vaccinated, and 3,155, or 20 percent, declined vaccination.
BWH offered several flu clinics this season for employees, and flu vaccinations continue to be available through OHS.
Karen Fiumara, PharmD, BCPS, director of Patient Safety and a task force member, said that the vaccination rate rose thanks to employees putting patients first and managers ensuring their employees were in compliance with the policy.
“I could not be more proud of the incredible progress we made,” Fiumara said. “What amazed me most is seeing how everyone came together to contribute to the success of the program. So many people have made extraordinary efforts to make the vaccine available and put the policy into operation. The task force is so thankful to employees who were vaccinated.”
Michael Calderwood, MD, MPH, of BWH Infection Control and the Division of Infectious Diseases and a member of the task force, said while the effectiveness of the flu vaccine can vary from year to year, flu vaccination typically reduces influenza incidence by 50 to 75 percent. He also said that, even when the vaccine is not a perfect match, those who are vaccinated and get influenza can have less severe illness.
The task force has begun working on plans for the 2016–2017 flu season and needs your input. Click here to participate in an anonymous survey. If you haven’t received flu vaccination, you can schedule your appointment by calling OHS at 617-732-6034. Learn more.






 B
B












 B
B









 P
P




 B
B BWH and the Department of Radiology mourn the loss of Beatrice Trotman-Dickenson, MBBS, who passed away on Dec. 3 after a short illness. She was 57.
BWH and the Department of Radiology mourn the loss of Beatrice Trotman-Dickenson, MBBS, who passed away on Dec. 3 after a short illness. She was 57.