
Behind the Scenes at the Brigham: Audiovisual Services

From left: Christopher Fenton and James Crowley manage audio and video broadcasts in the Zinner Breakout Room and Zinner Boardroom.
High-definition video of face-transplant surgery. Aerial footage of the helipad. Livestreamed events with hundreds of webcast viewers. These are just a few examples of the highly creative work produced by the Brigham’s Audiovisual Services (A/V) team in Office Services, which comprises several talented videographers, photographers, technicians and administrators who support every major service line and department.
“Our work is really fulfilling and fun,” said Peter Linck, manager of Office Services, which is part of Materials Management. “We get to work with so many people, and we also have a lot of creative freedom; when someone dreams up an audiovisual idea, we can help make it happen.”
And they do just that. Often spotted behind a camera or soundboard, the team supports dozens of events and multimedia projects in any given week. One moment, they could be broadcasting a hospital-wide event like Town Meeting or a tribute to the Rev. Dr. Martin Luther King Jr. from the A/V booth in Bornstein Amphitheater. The next, they could be filming neurosurgery cases in the Operating Rooms.
In addition to providing audio and video services, the team also assists the Brigham community with room reservations and event bookings. To make it easier for staff to determine the right venue for their event, the A/V team has made interactive, 360-degree online “tours” of many common meeting spaces, including the Zinner Conference Center and the Hale Building for Transformative Medicine.

From left: Elton Toska, Steven Kyriakidis, James Crowley, Benjamin Lee, Angel Ayala and Christopher Fenton (not pictured: John Bourque)
When all-hands requests arise, Linck enlists the help of their colleagues in the Mailroom, which also sits under the Office Services umbrella, to assist with coverage needs. He noted that everyone on the team works to expand their skillset and is eager to lend a hand—including being willing, at a moment’s notice, to support press conferences and large events, such as the Magnet celebration and Discover Brigham.
Many A/V staffers began their careers in the Brigham’s Mailroom and have diverse professional and freelance backgrounds spanning television, photography and graphic design. Also noteworthy is the team’s retention rate. Many have been part of A/V for over a decade, with the longest-tenured member, John Bourque, coordinator in Office Services, celebrating 39 years at the Brigham.
Angel Ayala, senior technician in Office Services, credits Linck with reinforcing the Brigham’s culture of innovation, collaboration, excellence and treating setbacks as opportunities to grow together—fostering an environment that Ayala says inspires the team to do their best every day.
“We have a really great, understanding manager who supports our growth,” he said, adding that whatever technology and skills are needed for the job—such as video adapters, GoPros, software tools and HTML programming classes—Ayala and his teammates are given what they need to produce high-quality content and provide exceptional service to the Brigham community.
“Behind the Scenes at the Brigham” is a monthly photo series in Brigham Bulletin that provides a glimpse of the people whose everyday contributions help make the Brigham a world-class institution. Is there an individual or team you’d like to see featured? Send your ideas to BWHBulletin@partners.org.
 Last summer, faculty and staff were invited to share their impressions of the Brigham’s organizational culture through the Brigham Experience: Culture, Diversity & Inclusion Assessment survey, focus groups, interviews and more. The message was clear: Our foundation and our people are strong, and we have opportunity to do even better, together.
Last summer, faculty and staff were invited to share their impressions of the Brigham’s organizational culture through the Brigham Experience: Culture, Diversity & Inclusion Assessment survey, focus groups, interviews and more. The message was clear: Our foundation and our people are strong, and we have opportunity to do even better, together.




 “When I got that diagnosis, it hit me like a brick. I thought, wow, there’s something else going on,” she said. “Genetically speaking, there’s no explanation for it.”
“When I got that diagnosis, it hit me like a brick. I thought, wow, there’s something else going on,” she said. “Genetically speaking, there’s no explanation for it.”
 Brigham Health’s Strategy in Action: Advanced, Expert Care
Brigham Health’s Strategy in Action: Advanced, Expert Care
 Researchers found the strongest associations were related to mood and self-harm. Those who slept less than six hours were more than three times as likely to consider or attempt suicide, and they were four times as likely to report an attempted suicide that resulted in treatment. Only 30 percent of the students in the study reported averaging more than eight hours of sleep on school nights.
Researchers found the strongest associations were related to mood and self-harm. Those who slept less than six hours were more than three times as likely to consider or attempt suicide, and they were four times as likely to report an attempted suicide that resulted in treatment. Only 30 percent of the students in the study reported averaging more than eight hours of sleep on school nights.









 “It was one of those seemingly inconsequential moments that he probably doesn’t remember, but I will never forget,” said LaMay.
“It was one of those seemingly inconsequential moments that he probably doesn’t remember, but I will never forget,” said LaMay.



 One example of how these rounds led to improved care involved a patient with a serious brain injury who spent one year at the Brigham as an inpatient.
One example of how these rounds led to improved care involved a patient with a serious brain injury who spent one year at the Brigham as an inpatient.
 Massachusetts has been one of the states hit hardest by the nation’s opioid crisis, with the rate of opioid-related deaths seeing a fourfold increase between 2000 and 2015 across the state. In the span of just one year, 2013 to 2014, opioid-related deaths occurred in two-thirds of cities and towns in Massachusetts, according to the state Department of Public Health.
Massachusetts has been one of the states hit hardest by the nation’s opioid crisis, with the rate of opioid-related deaths seeing a fourfold increase between 2000 and 2015 across the state. In the span of just one year, 2013 to 2014, opioid-related deaths occurred in two-thirds of cities and towns in Massachusetts, according to the state Department of Public Health.
 When the ED is at capacity, some patients leave after being seen by a triage nurse, but before being seen by a physician. When a “walkout” occurs – often due to long wait times – it not only leads to a poor patient experience, but it is also a safety concern, as nearly 30 percent of patients who receive care in the Brigham’s ED are sick enough to be admitted.
When the ED is at capacity, some patients leave after being seen by a triage nurse, but before being seen by a physician. When a “walkout” occurs – often due to long wait times – it not only leads to a poor patient experience, but it is also a safety concern, as nearly 30 percent of patients who receive care in the Brigham’s ED are sick enough to be admitted.

 Mohamed El-Dib, MD, director of Neonatal Critical Care in the Department of Pediatric Newborn Medicine, is the principal investigator at BWH for a multi-institutional clinical trial looking at whether infusing babies with their own umbilical cord blood can indeed reverse tissue damage in the brain.
Mohamed El-Dib, MD, director of Neonatal Critical Care in the Department of Pediatric Newborn Medicine, is the principal investigator at BWH for a multi-institutional clinical trial looking at whether infusing babies with their own umbilical cord blood can indeed reverse tissue damage in the brain.
 NICU staff also attended multidisciplinary workshops last fall hosted by the team, which incorporated training videos for staff that depicted various clinical scenarios, including how to properly perform hand hygiene and sterile tubing line changes. They also demonstrated collegial ways to approach someone who had not performed hand hygiene and was attempting to touch a patient.
NICU staff also attended multidisciplinary workshops last fall hosted by the team, which incorporated training videos for staff that depicted various clinical scenarios, including how to properly perform hand hygiene and sterile tubing line changes. They also demonstrated collegial ways to approach someone who had not performed hand hygiene and was attempting to touch a patient.
 “A patient may come to the Neurosurgery clinic for an appointment, and, after reviewing a case, we realize having one of our ENT specialists join us would be ideal,” Dunn said. “That can happen in real time rather than after scheduling a visit in another two weeks. It can be difficult for patients to return for multiple appointments, so we’re trying to deliver everything on site at once.”
“A patient may come to the Neurosurgery clinic for an appointment, and, after reviewing a case, we realize having one of our ENT specialists join us would be ideal,” Dunn said. “That can happen in real time rather than after scheduling a visit in another two weeks. It can be difficult for patients to return for multiple appointments, so we’re trying to deliver everything on site at once.”



 The website provides easy access to an extensive array of BWH departments and services, including Information Services (IS), Security, environmental chemical waste collection, Interpreter Services, Audiovisual Services and more.
The website provides easy access to an extensive array of BWH departments and services, including Information Services (IS), Security, environmental chemical waste collection, Interpreter Services, Audiovisual Services and more.
 During his treatment, however, other aspects of Thurber’s health began to deteriorate. He couldn’t walk. He needed supplemental oxygen to breathe. Baffled by this sharp decline, Thurber’s physicians recommended he go to Boston to see specialists at BWH.
During his treatment, however, other aspects of Thurber’s health began to deteriorate. He couldn’t walk. He needed supplemental oxygen to breathe. Baffled by this sharp decline, Thurber’s physicians recommended he go to Boston to see specialists at BWH.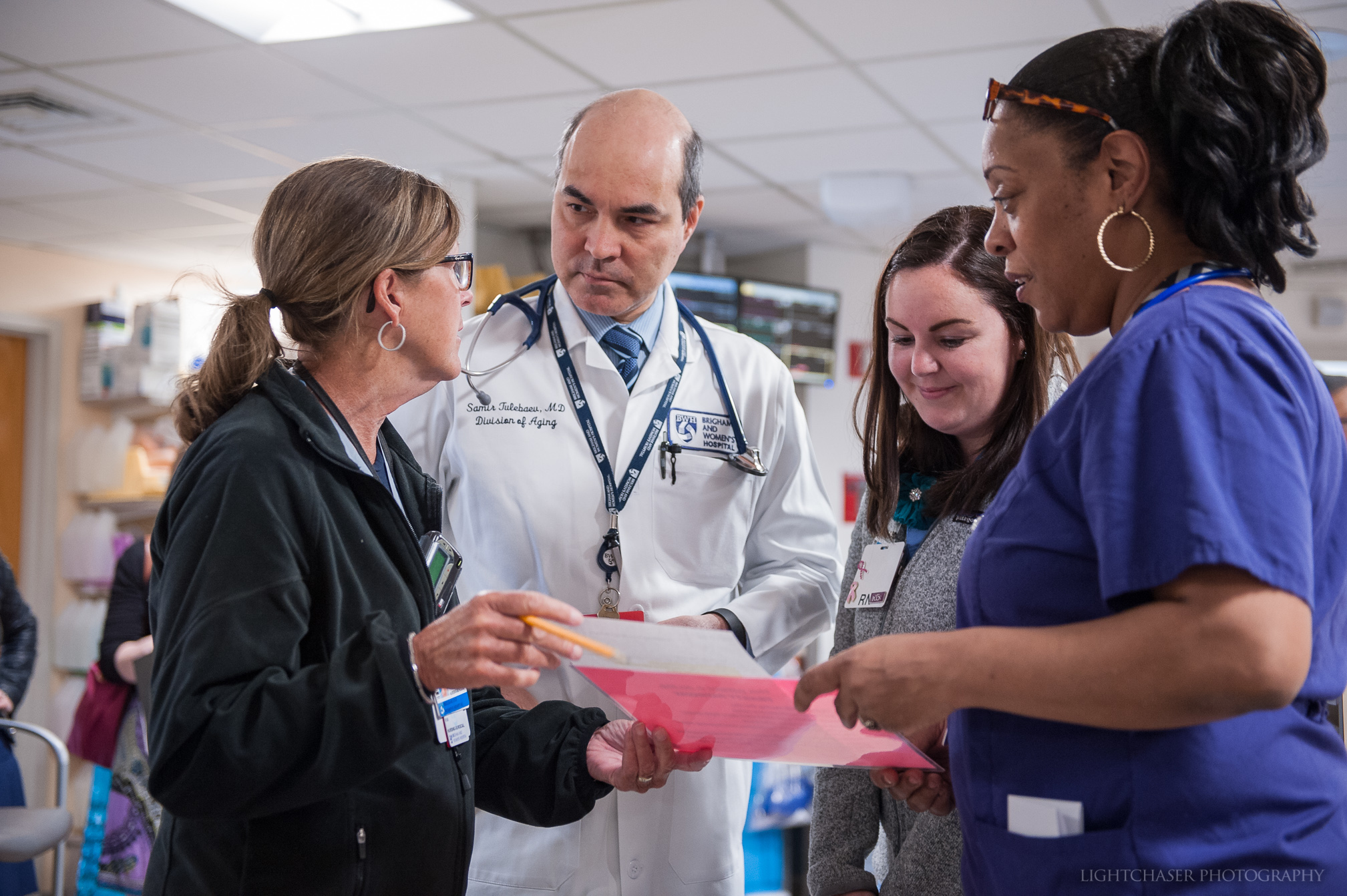
 As part of this journey, staff are invited to contribute to an interactive display in the 75 Francis St. lobby by sharing how they exemplify four hallmarks of Magnet institutions – high-quality patient care, clinical excellence, innovations in professional practice and interprofessional collaboration – in their daily work. Stickers provided at a nearby table encourage staff to write about how their role exemplifies one or more of those categories.
As part of this journey, staff are invited to contribute to an interactive display in the 75 Francis St. lobby by sharing how they exemplify four hallmarks of Magnet institutions – high-quality patient care, clinical excellence, innovations in professional practice and interprofessional collaboration – in their daily work. Stickers provided at a nearby table encourage staff to write about how their role exemplifies one or more of those categories. The Weiner lab has an ambitious goal: to develop a nasal vaccine that will prevent and reverse the progression of Alzheimer’s disease.
The Weiner lab has an ambitious goal: to develop a nasal vaccine that will prevent and reverse the progression of Alzheimer’s disease.
 Pharmacy students on the team have a lot of face-to-face conversations with patients about medication management. Students counsel patients about their medications and assess barriers to medication adherence.
Pharmacy students on the team have a lot of face-to-face conversations with patients about medication management. Students counsel patients about their medications and assess barriers to medication adherence. In April, BWH submitted evidence of the hospital’s commitment to quality patient care, clinical excellence, interprofessional collaboration and innovation for consideration as a Magnet-designated hospital. While the Magnet Recognition Program’s roots are in nursing, the designation honors the work and culture of an entire institution.
In April, BWH submitted evidence of the hospital’s commitment to quality patient care, clinical excellence, interprofessional collaboration and innovation for consideration as a Magnet-designated hospital. While the Magnet Recognition Program’s roots are in nursing, the designation honors the work and culture of an entire institution.
 Pointing to a recent cohort study and findings from randomized clinical trials, Manson said that there is an increasingly strong case for the link between the heart and brain. Traditional heart disease risk factors – smoking, hypertension, high cholesterol, diabetes and obesity – were found to correlate with the presence of amyloid plaques in the brain, a protein whose buildup is associated with Alzheimer’s.
Pointing to a recent cohort study and findings from randomized clinical trials, Manson said that there is an increasingly strong case for the link between the heart and brain. Traditional heart disease risk factors – smoking, hypertension, high cholesterol, diabetes and obesity – were found to correlate with the presence of amyloid plaques in the brain, a protein whose buildup is associated with Alzheimer’s.
 Investigators found that a single measurement of a novel biomarker for diabetes known as plasma glycated CD59 (GCD59), performed at weeks 24-28 of gestation, was able to identify women who had failed the standard of care screening test as well as women with confirmed gestational diabetes. The findings were published in a recent issue of Diabetes Care.
Investigators found that a single measurement of a novel biomarker for diabetes known as plasma glycated CD59 (GCD59), performed at weeks 24-28 of gestation, was able to identify women who had failed the standard of care screening test as well as women with confirmed gestational diabetes. The findings were published in a recent issue of Diabetes Care.