New Brigham Spine Center Simplifies, Enhances Access to Spinal Care

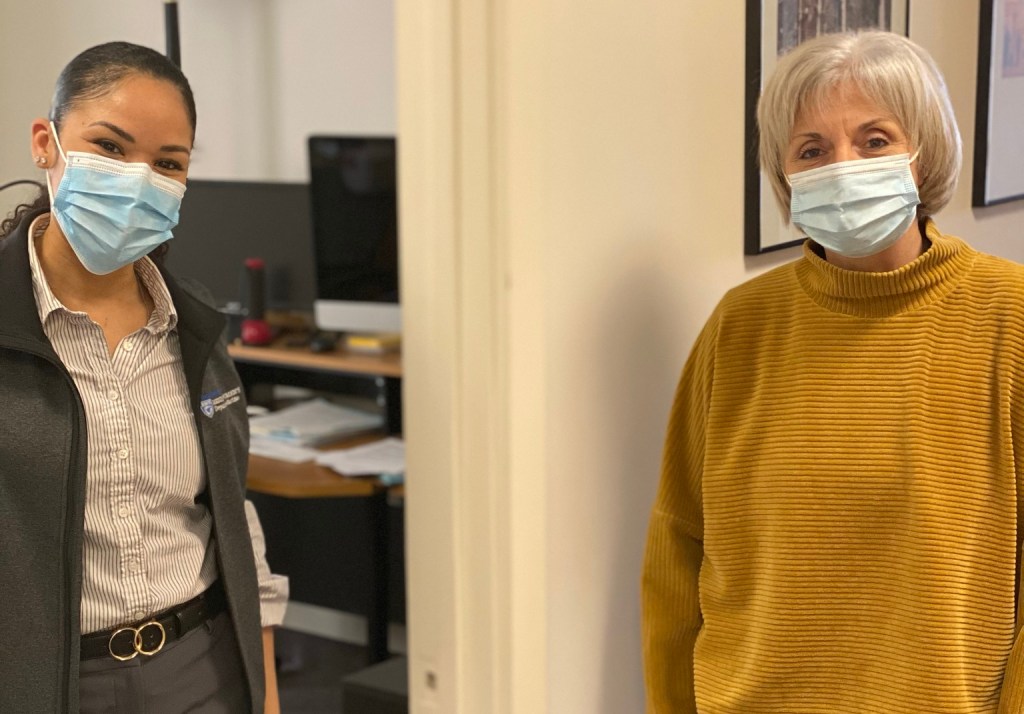
“This co-location is a super-charger in terms of exchanging ideas and information,” says pain medicine specialist Christopher Gilligan (right), shown discussing a recent case with orthopaedic spine surgeon Melvin Makhni (left).
After completing a long-distance run last year, Wendy started to feel pain radiating from her lower back into her legs. Within days, she couldn’t walk, let alone run. Even sitting — something she did for 10 hours a day at work — became excruciating.
Oh, no, she thought. Not again.
 Wendy (who requested her last name not be used) had experienced a debilitating back injury several years prior. Although the location of the pain was different this time, its severity was all too familiar. And as someone who thrived in an active lifestyle, her heart sank at the possibility of having her mobility compromised again.
Wendy (who requested her last name not be used) had experienced a debilitating back injury several years prior. Although the location of the pain was different this time, its severity was all too familiar. And as someone who thrived in an active lifestyle, her heart sank at the possibility of having her mobility compromised again.
Fortunately, she knew exactly whom to call: James Kang, MD, chair of the Department of Orthopaedic Surgery, who led the team that performed her last back surgery about four years ago.
After Wendy underwent an X-ray and MRI for her more recent issue, she expected Kang to start discussing options for another surgery, but the direction of their conversation surprised her. He suggested she meet with Christopher Gilligan, MD, MBA, chief of the Division of Pain Medicine, to see if epidural injections would sufficiently manage her back pain.
At first, Wendy acknowledged, she was skeptical. With her first back injury, specialists at other institutions had recommended injections, which were ultimately unsuccessful. On the other hand, she wasn’t eager to undergo another surgery. Wendy said she put her trust in her Brigham care team, and, sure enough, the injections resolved her pain and restored her function.
“It’s a thousand times better,” she said. “I’m back to running three miles a day, going to yoga and Pilates, and doing Crossfit. I’m also training for the Pan Mass Challenge and actually just did a 50-mile bike ride a couple of weeks ago, too.”
It wasn’t just the quality of care and speed of her recovery that amazed her, Wendy says. The seamless collaboration her providers demonstrated, and the ease with which staff swiftly managed her referrals and insurance approvals, left a lasting impression as well.
“As the patient, you’re already exhausted and in pain. The last thing you want to do is run around and find out who to see next,” Wendy said. “My doctors and their staff bend over backwards to coordinate with each other, and they try to find every possible solution and see what someone else may have missed.”

“It’s a thousand times better,” says Wendy, who is back to doing what she loves most — staying active — after undergoing epidural injections in her lower back.
That’s exactly the experience that Gilligan says every patient can expect to receive at the Brigham and Women’s Spine Center, a new service line that seeks to enhance spine care through improved multidisciplinary collaboration, expanded and more timely access to care, and a more seamless experience for patients and referring providers.
“When a patient has neck or back pain, there are a lot of different types of specialists they could see. How would they know who’s the right one for their concern? That complexity is a real and understandable source of frustration for patients,” said Gilligan, who serves as director of the new Spine Center. “We’re taking the burden of navigation off patients and referring providers. All they need to do is call or email the Spine Center, and we’ll take care of the rest. We’ll get them to the right provider at the right place at the right time.”
A Collaboration ‘Super-Charger’
With a combined team of neurosurgeons, orthopaedic surgeons, pain medicine specialists, physical medicine and rehabilitation specialists, advanced practitioners and other clinical staff, the Spine Center delivers integrated care and innovative treatments for spine patients.
“We may all see the same type of patient, but we each have different tools in our toolbox,” said Spine Center neurosurgeon Hasan Zaidi, MD, who also serves as co-director of the Adult Spinal Deformity and Scoliosis Program. “The best way to support our patients is to put all these great minds together, which we’ve been doing for years. Now we are strengthening our collaboration even more with the launch of this Spine Center.”
It’s far more common for these specialists to have clinics independent from one another, Gilligan said, but the Spine Center is based on the notion that multidisciplinary collaboration between these providers is essential to providing the best care. That’s why one of the center’s founding objectives is to have surgical and non-surgical providers “co-located” in, or share, the same physical workspace.
“We write our notes sitting next to each other in the same physician workroom. We’re looking at the patient’s MRI together. We’re talking about their case together,” Gilligan said. “This co-location is a super-charger in terms of exchanging ideas and information.”
To improve access to care, the Spine Center provides services at 10 locations, including the main campus in the Hale Building for Transformative Medicine as well as sites in Chestnut Hill, Foxborough, Framingham, Jamaica Plain, Milford, Mansfield, Pembroke, South Weymouth and Westwood. The team also includes several physician assistants who specialize in spinal care to expand access and reduce wait times.
“This is such an extraordinarily talented team with an outstanding depth of quality in different fields. To my mind, the level of spine expertise we have at the Brigham is unmatched,” Gilligan said. “I’m incredibly enthusiastic about the many ways in which we’ll provide patients with enhanced care while just making it that much simpler for patients to get the care they need.”
To contact the Spine Center, call 877-777-2134. For an e-referral, Brigham providers can use the Epic referral name “BWH Spine Center.”

 Sydney Sanford, head of the Child Life Program in Radiation Oncology, was one of the first individuals Shadiamond encountered upon beginning treatment. An expert at easing nerves and bringing lightheartedness to high-stress situations, particularly for younger patients, Sanford quickly became a friendly, familiar face to Shadiamond and her family.
Sydney Sanford, head of the Child Life Program in Radiation Oncology, was one of the first individuals Shadiamond encountered upon beginning treatment. An expert at easing nerves and bringing lightheartedness to high-stress situations, particularly for younger patients, Sanford quickly became a friendly, familiar face to Shadiamond and her family.


























































 “As tight-knit as we were on the General Medicine units, the COVID teams have made us even closer,” said Kelly-Makol, who has been part of the PACE Service for eight years. “When we were starting to provide care on the Special Pathogens Unit, there was a lot of anxiety. We started this group text that became a stream-of-consciousness thread for our thoughts, concerns and occasionally humor. It kept us all smiling and feeling like we weren’t alone.”
“As tight-knit as we were on the General Medicine units, the COVID teams have made us even closer,” said Kelly-Makol, who has been part of the PACE Service for eight years. “When we were starting to provide care on the Special Pathogens Unit, there was a lot of anxiety. We started this group text that became a stream-of-consciousness thread for our thoughts, concerns and occasionally humor. It kept us all smiling and feeling like we weren’t alone.”
 Since the arrival of COVID-19, the PACE Service has played a vital role in pandemic response. But when the spring 2020 surge set in, the teams quickly realized they needed more help. To manage the sharp increase in patient volume and complexity during the initial surge, about 40 PAs from other areas of the hospital were temporarily reassigned to the PA Special Pathogen Teams.
Since the arrival of COVID-19, the PACE Service has played a vital role in pandemic response. But when the spring 2020 surge set in, the teams quickly realized they needed more help. To manage the sharp increase in patient volume and complexity during the initial surge, about 40 PAs from other areas of the hospital were temporarily reassigned to the PA Special Pathogen Teams.