Wave of Innovation Occurs in the Fight Against COVID-19
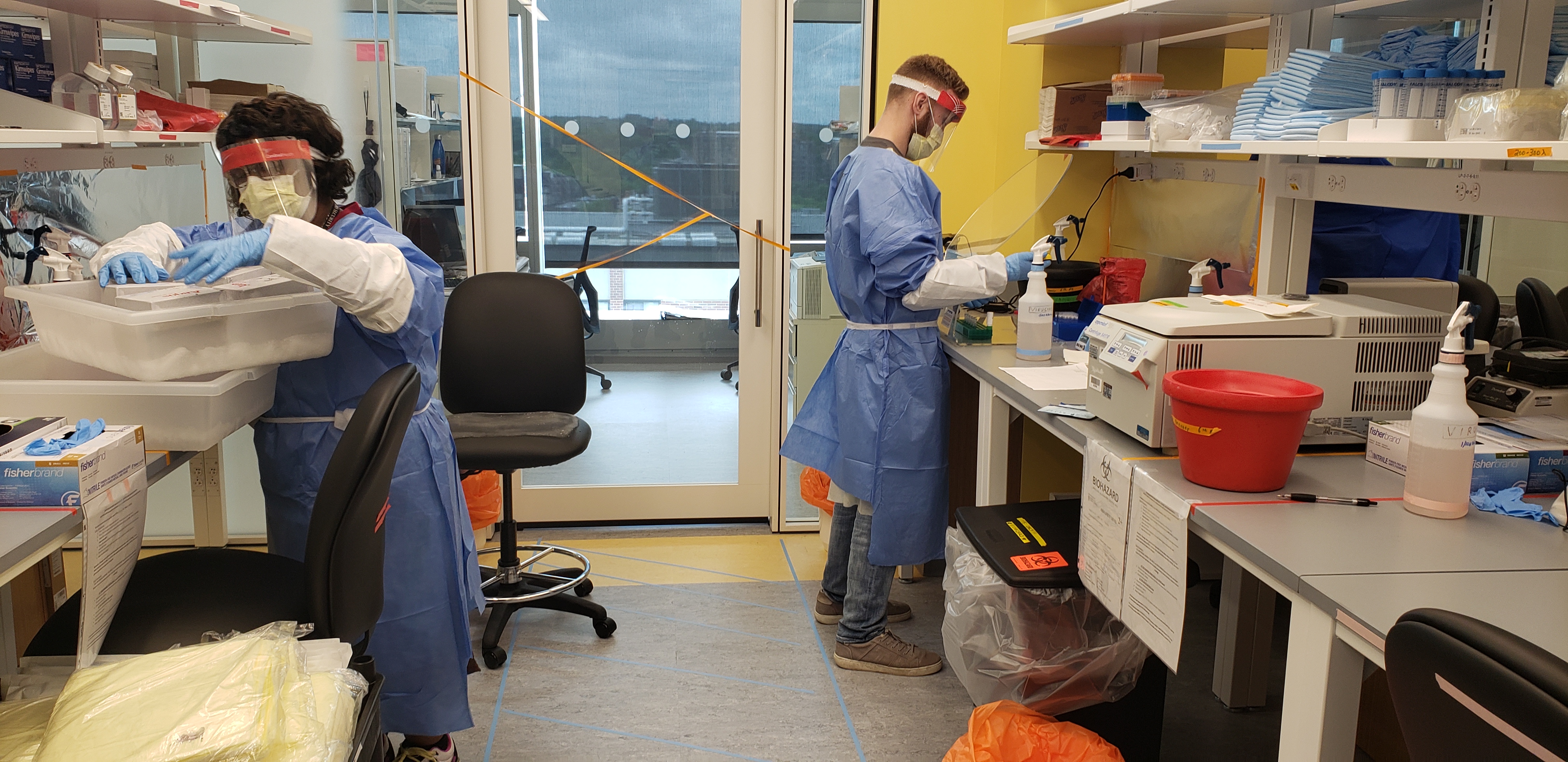
From left: Vannessa Davis and Samuel Bates support the MGB Center for COVID Innovation’s Diagnostic Accelerator.
With expertise that spans basic, translational and clinical research, Brigham clinicians and investigators have been working tirelessly to address the most urgent needs related to the COVID-19 pandemic.
To help reduce the spread of COVID-19, the Brigham shut down most of its physical research labs from March through the beginning of June. But even during the shutdown, many labs continued their work remotely and new efforts began to better understand the virus that causes COVID-19 (SARS-CoV-2), and the nature of the pandemic itself, in order to develop treatment strategies against them.
“In mid-March, hundreds of Brigham investigators and laboratory staff quickly pivoted to contribute to COVID-19 research and addressing COVID-related problems,” said Jacqueline Slavik, PhD, MSc, executive director of the Brigham Research Institute (BRI). “Within days, Brigham investigators were launching clinical trials, developing safer testing procedures and solving problems around personal protective equipment (PPE) shortages.”
Throughout the pandemic, Brigham investigators continued to pursue and receive funding for COVID-19 research — including clinical studies for a variety of potential therapies — through government and industry grants.
“Thanks to incredible ingenuity, a strong foundation and a breadth of core resources, our research community remains remarkably successful at putting forward award-winning research proposals and conducting first-class research,” said Paul Anderson, MD, PhD, chief academic officer and senior vice president of Research and Education. “As our research enterprise ramps up, these awards will become more important than ever, not only for individual research labs but also for the larger world as we continue to combat this pandemic.”
A Wave of New Solutions for COVID-19

Anesthesiologist Greg Crosby wears a 3D-printed face shield. Photo credit: Jim Rathmell, MD
Clinicians and researchers from the Brigham have come together with colleagues from around the world to produce a wave of innovative solutions faster than ever before.
Some of the Brigham’s advances in the fight against COVID-19 include:
- Developing an innovative testing strategy to conserve PPE: A Brigham team developed the Brigham Protective Equipment for Clinical Test Environment and Diagnostics (B-PROTECTED) booth to preserve PPE and protect clinicians from COVID-19.
- Creating in-house COVID-19 testing with results available within 24 hours: Brigham investigators implemented a rapid in-house test for COVID-19 patients who’ve been admitted to the Brigham but don’t yet have a definitive diagnosis.
- Designing new face shields to protect health care workers from infection: A team of clinicians at the Brigham worked with academic and industry partners to design and develop a new 3D-printed face shield that offers a number of advantages over traditional shields.
- Developing new protective materials: The lab of Jeff Karp, PhD,is working on an extended-duration sanitizer and a nasal spray to form a shield that protects against inhaled pathogens and viruses.
- Investigating a safer way to split ventilators: Pulmonary physicians and biomedical engineers have been working together to develop a system that can be built from off-the-shelf components to allow for patient-specific volume and pressure control when using a single ventilator for more than one patient.
- Using sewage to map an outbreak: Physician-investigators Peter Chai, MD, and Tim Erickson, MD, both of the Division of Medical Toxicology, are working with collaborators to develop technology and a plan for sampling sewage in North Carolina and Boston. These samples may provide important clues about the presence or absence of SARS-CoV-2 over time.
- Investigating connections during social distancing: The lab of Amar Dhand, MD, DPhil, of the Department of Neurology, is researching the connections between individuals and their social networks. The team is learning firsthand how to stay connected during the time of social distancing.
- Developing a universal coronavirus vaccine: The lab of Thomas Kupper, MD, chair of the Department of Dermatology, is investigating a vaccine that may protect against COVID-19 along with past, current and future strains of coronavirus.

Shriya Srinivasan and colleagues are working on a safer way to split ventilators
“It’s inspiring to see how highly collaborative the Brigham research community has been during this crisis,” said Slavik. “Our research efforts have involved countless individuals from many academic institutions, the technology sector, industry and private companies — all of whom are working towards the common goal of mitigating COVID-19.”
Clinical Studies to Understand, Treat and Prevent COVID-19
To better understand COVID-19 and the virus that causes it, investigators are working on a range of studies and trials. These include:
- Remdesivir clinical trials: The Brigham is a clinical trial site for evaluating the antiviral medication remdesivir in patients with COVID-19.
- Learning from patients who’ve recovered from COVID-19: The lab of Duane Wesemann, MD, PhD, of the Division of Immunology and Allergy, is testing blood samples from people who’ve recovered from infection. These samples will help the team learn more about rates of exposure, the types of antibodies an infection elicits and the degree of immunity recovered patients have against re-infection.
“The Brigham has also created a COVID-19 biorepository to collect an array of biospecimens from patients who are or have been COVID-positive,” said Allison Moriarty, MPH, vice president of Research Administration and Compliance. “We believe this biorepository will be a key tool in helping us learn how to detect, treat and prevent COVID-19 in the future.”
A New Center for COVID Innovation
To rapidly develop new innovations and protect frontline staff across the Mass General Brigham (MGB) community and beyond, colleagues at Massachusetts General Hospital (MGH) and the Brigham research community launched the Mass General Brigham Center for COVID Innovation (MGBCCI) in March.
 “The mission of the MGB Center for COVID Innovation is to organize and consolidate the rapid investigation and clinical deployment of devices, diagnostics, data, analytics and the therapeutics that MGH and the Brigham is generating to combat the COVID-19 crisis,” center co-director said David Walt, PhD, a medical diagnostics researcher at the Brigham and Harvard University’s Wyss Institute for Biologically Inspired Engineering.
“The mission of the MGB Center for COVID Innovation is to organize and consolidate the rapid investigation and clinical deployment of devices, diagnostics, data, analytics and the therapeutics that MGH and the Brigham is generating to combat the COVID-19 crisis,” center co-director said David Walt, PhD, a medical diagnostics researcher at the Brigham and Harvard University’s Wyss Institute for Biologically Inspired Engineering.
Investigators at the MGBCCI directly responded to, and continue to address, the most pressing needs that face health care workers — prototyping and testing new PPE, patient isolation hoods, alternative versions of respirators, face masks, face shields and nasal swabs.
Working groups within the MGBCCI have already identified and developed several new devices. They’re exploring other potential solutions for problems related to the pandemic. These efforts include:
- Improving surgical mask design: The surgical masks group identified design inputs and criteria that are being applied to the design of an “ideal” surgical mask to improve upon the current design.
- Reusing ventilators: The ventilators team is investigating the potential disinfection and reuse of HME/HEPA ventilator filters. They’re also working with software engineers to build a remote monitoring and alarm system for ventilators.
- Replacing N95 respirators with novel devices: The N95 respirators team is exploring novel ideas for devices that could replace N95 respirators that aren’t dependent on the filtration media supply chain. They also developed a way to repair 50,000 defective N95 respirators with New Balance.
“We’re also working to identify a direct-to-consumer diagnostic test that could be used at home. When implemented, people can quarantine themselves if they are positive for COVID-19,” said Walt. “These tests could help stem flare-ups of COVID-19 cases that will invariably happen when people return to work and reintegrate into society.”