
Brigham Named on U.S. News Honor Roll, OB-GYN Ranks as #1 in Nation Again
![]() Brigham and Women’s Hospital was named one of the nation’s top hospitals by U.S. News & World Report in its 2023–24 “Best Hospitals” list and ranked first nationwide for Obstetrics and Gynecology for the second year in a row.
Brigham and Women’s Hospital was named one of the nation’s top hospitals by U.S. News & World Report in its 2023–24 “Best Hospitals” list and ranked first nationwide for Obstetrics and Gynecology for the second year in a row.
Each year, U.S. News performs a comprehensive, nationwide evaluation of adult specialties, recognizing the country’s leading hospitals and specialties and other high-performing hospitals that provide exceptional care. This year, U.S. News & World Report announced several changes to their methodology, including the elimination of ordinal ranking from this year’s Honor Roll. U.S. News will continue to publish ordinal rankings of the 15 specialties it evaluates and for specific regions.
The Brigham ranked in 12 of the 13 specialties it is eligible to be ranked in, and this year marked improvements in five specialties. In addition to the top ranking for OB-GYN, Dana-Farber Brigham Cancer Center ranked fifth in cancer, and BWH Rheumatology ranked fifth nationwide as well. Additionally, the Brigham earned U.S News’ highest distinction in 18 of the 21 common medical conditions and procedures that are evaluated.
“These rankings reflect the incredible commitment and talent of our Brigham community,” said Robert S.D. Higgins, MD, MSHA, president of the Brigham and executive vice president at Mass General Brigham. “And while it is always gratifying to be recognized in this manner, what fills me with the greatest pride is the exceptional and compassionate care we deliver to our patients and their loved ones every day by upholding our shared values.”
Nawal Nour, MD, MPH, chair of the Department of Obstetrics and Gynecology, said achieving this national recognition was especially meaningful given the current landscape surrounding women’s health.
“We are thrilled to be recognized as the top OB-GYN department in the country for the second consecutive year,” Nour said. “As we face sobering statistics nationally regarding women’s reproductive health and maternal mortality, we are proud of the incredible work of our team in not only providing excellent patient care but also working every day to protect the health of some of our most vulnerable patients. Our clinical care team ensures our high-quality, comprehensive care is tailored to each stage of the patient health journey.”
The annual ratings were developed to help consumers determine which hospitals provide the best care for challenging or complicated health conditions and for common elective procedures. They are based on a point system derived from a comprehensive nationwide evaluation of nearly 5,000 medical centers in 15 adult specialties and 21 procedures and conditions.
Across the system, Mass General Brigham hospitals continued to earn top honors. Massachusetts General Hospital also earned a spot on the Honor Roll of the best hospitals in the country once again. McLean Hospital was No. 1 in the nation in Psychiatry, followed by MGH at No. 2. Spaulding Rehabilitation ranked No. 2 in the nation for Rehabilitation, while Mass Eye and Ear ranked No. 4 in the nation for Ophthalmology and No. 7 for Otolaryngology. Our community hospitals continue to earn high marks in regional rankings.
Earlier this year, Mass General Brigham launched For Every Patient, a systemwide unified quality strategy that seeks to achieve the best possible outcomes for every patient. For Every Patient is a multi-year, evidence-based, data-driven effort that will provide high-quality care that is effective, safe, personalized and rooted in equity at every touchpoint, for every patient.
Additional details about the U.S. News & World Report ranking system can be found here. The complete listing of America’s Best Hospitals can be found here.
By the Numbers: 2023 Rankings by Specialty

*Brigham is not ranked in Ophthalmology or Rehabilitation. Mass Eye and Ear, which is tied to MGH for Honor Roll Purposes, ranked No. 4 for Ophthalmology. Spaulding, which is tied to MGH for Honor Roll purposes, ranked No. 2 for rehabilitation.

 Brigham and Women’s Hospital mourns the loss of Lawrence “Larry” Jones, ambulatory practice manager in the Division of Endocrinology, Diabetes and Hypertension, who died June 13 after an extended illness. He was 63.
Brigham and Women’s Hospital mourns the loss of Lawrence “Larry” Jones, ambulatory practice manager in the Division of Endocrinology, Diabetes and Hypertension, who died June 13 after an extended illness. He was 63.





 Brigham and Women’s Hospital mourns the loss of K. Frank Austen, MD, founding chief of the Division of Rheumatology, Immunology and Allergy at BWH and the AstraZeneca Professor of Respiratory and Inflammatory Diseases, Emeritus, at Harvard Medical School. Dr. Austen died on June 23 at the age of 95.
Brigham and Women’s Hospital mourns the loss of K. Frank Austen, MD, founding chief of the Division of Rheumatology, Immunology and Allergy at BWH and the AstraZeneca Professor of Respiratory and Inflammatory Diseases, Emeritus, at Harvard Medical School. Dr. Austen died on June 23 at the age of 95.








 Brigham and Women’s Hospital mourns the loss of Martin A. Samuels, MD, founding chair emeritus of the Department of Neurology and the Miriam Sydney Joseph Distinguished Professor of Neurology at Harvard Medical School, who died June 6. He was 77.
Brigham and Women’s Hospital mourns the loss of Martin A. Samuels, MD, founding chair emeritus of the Department of Neurology and the Miriam Sydney Joseph Distinguished Professor of Neurology at Harvard Medical School, who died June 6. He was 77.



























































 In recognition of the exemplary patient- and family-centered care that our Department of Obstetrics and Gynecology delivers, U.S. News & World Report named the Brigham the nation’s #1 hospital for Obstetrics and Gynecology. This recognition accompanied the news that the Brigham once again earned a spot on U.S. News’ Best Hospitals Honor Roll for 2022–23.
In recognition of the exemplary patient- and family-centered care that our Department of Obstetrics and Gynecology delivers, U.S. News & World Report named the Brigham the nation’s #1 hospital for Obstetrics and Gynecology. This recognition accompanied the news that the Brigham once again earned a spot on U.S. News’ Best Hospitals Honor Roll for 2022–23.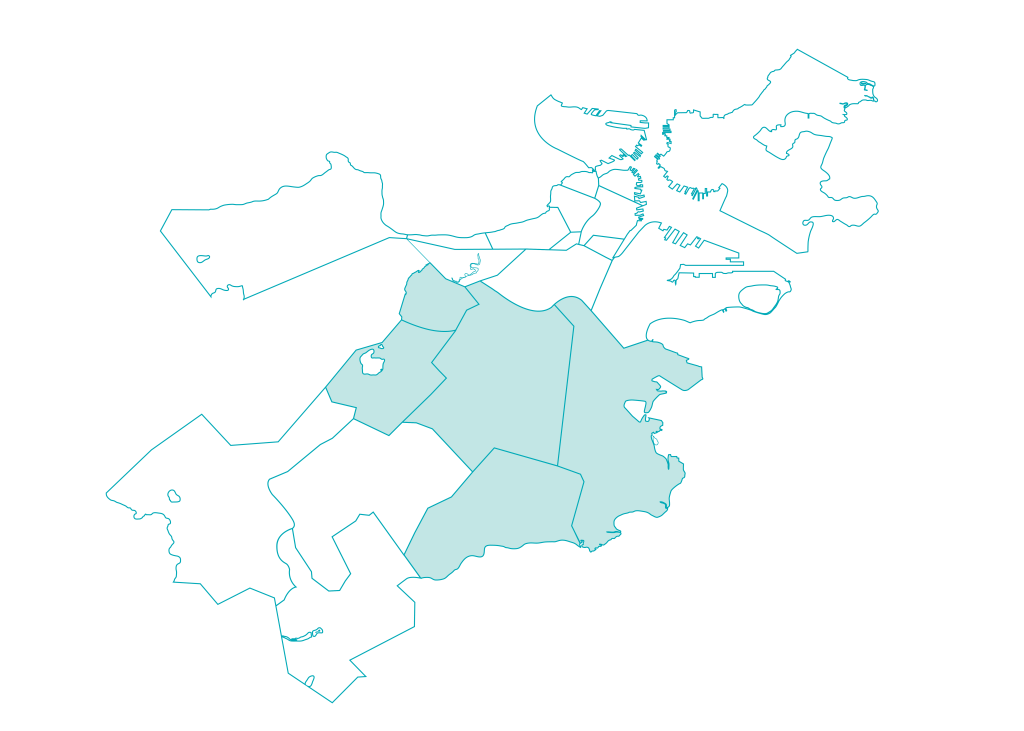 As part of our 2022 Community Health Assets and Needs Assessment, the Brigham participated in a citywide collaborative to jointly identify and address the most pressing health issues facing Boston residents. Guided by input from residents and local organizations in the Brigham’s five priority neighborhoods — Dorchester, Jamaica Plain, Mattapan, Mission Hill and Roxbury — we are partnering with community stakeholders to eliminate health inequities.
As part of our 2022 Community Health Assets and Needs Assessment, the Brigham participated in a citywide collaborative to jointly identify and address the most pressing health issues facing Boston residents. Guided by input from residents and local organizations in the Brigham’s five priority neighborhoods — Dorchester, Jamaica Plain, Mattapan, Mission Hill and Roxbury — we are partnering with community stakeholders to eliminate health inequities.

 Last summer, physician-scientists from the Brigham presented new evidence that drugs originally developed to treat type 2 diabetes may benefit a wide range of patients experiencing heart failure. Brigham investigators helped lead the largest clinical trial to date on a broad range of patients with heart failure, finding that a class of drugs known as SGLT2 inhibitors provided protection from cardiovascular events.
Last summer, physician-scientists from the Brigham presented new evidence that drugs originally developed to treat type 2 diabetes may benefit a wide range of patients experiencing heart failure. Brigham investigators helped lead the largest clinical trial to date on a broad range of patients with heart failure, finding that a class of drugs known as SGLT2 inhibitors provided protection from cardiovascular events.

 I am extraordinarily proud of all that we accomplished in 2022 to deliver expert and compassionate care, drive research and innovation, train tomorrow’s health care professionals and care for our communities.
I am extraordinarily proud of all that we accomplished in 2022 to deliver expert and compassionate care, drive research and innovation, train tomorrow’s health care professionals and care for our communities.







 Over the past year, I have quickly become aware of how special our health care providers — including nurses, doctors and other care team members — are in taking care of our patients and their families. And now through personal experiences for me and my family, I further recognize the high-quality and compassionate care our organization provides. Recognizing what all of our patients and their families already know, our Brigham family delivers world-class care with outstanding compassion and dedication to our community and its well-being. Thank you for all that you do.
Over the past year, I have quickly become aware of how special our health care providers — including nurses, doctors and other care team members — are in taking care of our patients and their families. And now through personal experiences for me and my family, I further recognize the high-quality and compassionate care our organization provides. Recognizing what all of our patients and their families already know, our Brigham family delivers world-class care with outstanding compassion and dedication to our community and its well-being. Thank you for all that you do.