
After 27 Years, and a Lot of Heart, Local Grandfather Achieves Lifesaving Milestone of 550 Platelet Donations at Kraft Center
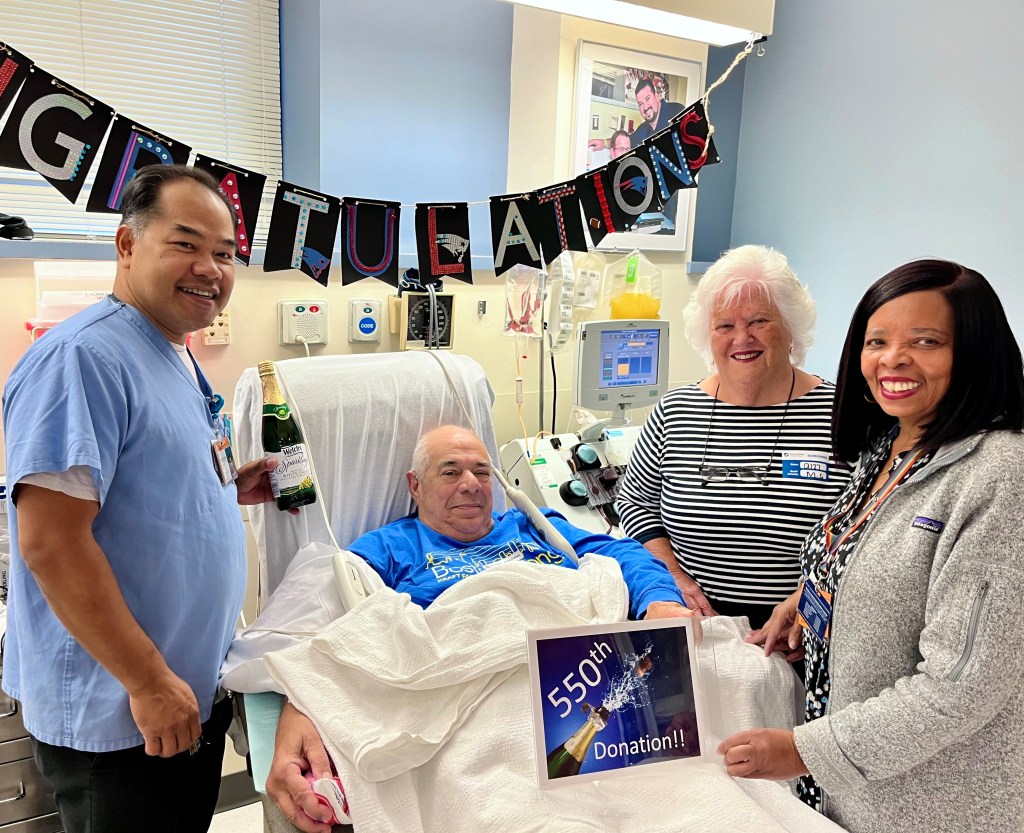
Ralph “Rocco” Russo (center left) celebrates his 550th blood platelet donation with his wife, Annemarie (center right), with members of the Kraft Center team, including Someth Em (left) and Marie Fleurant (right).
When his best friend’s then 14-year-old daughter was diagnosed with cancer in 1996, Ralph “Rocco” Russo said he gladly made his first blood platelet donation “because I needed to do whatever I could to help.”
The 77-year-old Marshfield grandfather, who has continued the practice for the past 27 years, recently celebrated his 550th platelet donation at Kraft Family Blood Donor Center which is celebrating its 40th anniversary providing lifesaving blood products to patients at Brigham and Women’s Hospital and Dana-Farber Cancer Institute.
Platelets act as the body’s bandages, allowing blood to clot and wounds to heal. Cancer patients and other critically ill patients often require transfusions of healthy platelets because their blood does not clot properly. Once donated, however, platelets have a shelf life of just five days.
“That’s why the need for donors is constant — and why donations on a magnitude like Rocco’s are so significant,” said Sean Stowell, MD, PhD, medical director of the Kraft Family Blood Donor Center and Transfusion Medicine at the Brigham.
It is estimated that Russo’s platelet donations, which he makes every other week, have amounted to 69 gallons of blood products and, consequently, contributed to saving 550 lives.
“I’ve been going to the Kraft Center for a third of my life, so it’s my second home. Everyone is so nice, and the donation process doesn’t hurt,” Russo said. “I know donating helps a lot of people, and it’s a walk in the park for me.”
Among the “many great people” Russo said he has met over the years is a man whose bone marrow cancer went into remission a few years ago following treatments that included an infusion of his type-O positive blood. In addition, Russo said he was touched that the celebration of his 300th platelet donation in December 2011 was attended by Nicole Sorensen, whose childhood illness inspired his activism so many years ago.
Sorensen, a chef in the food service industry, was studying to be a nurse when she passed away on May 17, 2012 — one day after her 39th birthday. Russo said he will continue to donate platelets “for as long as I’m able” in her honor.
“Rocco’s selfless dedication to helping others has always been deeply admired and appreciated,” said Molly McDermott, recruitment program manager at the Kraft Family Blood Donor Center. “His commitment — and that of all our donors — is especially important now to ensure that our patients may continue receiving essential medical care.”
Donors can make an appointment to give blood or platelets at the Kraft Family Blood Donor Center (open Tuesday through Sunday) by calling 617-632-3206 or emailing BloodDonor@partners.org. Walk-ins are welcome at the center, which is located at 35 Binney St.







 Dr. Jonathan Leong, undeterred by a devastating diagnosis of a glioblastoma in 2017, was a beloved and dedicated intern in the Brigham’s Internal Medicine Residency Program until his
Dr. Jonathan Leong, undeterred by a devastating diagnosis of a glioblastoma in 2017, was a beloved and dedicated intern in the Brigham’s Internal Medicine Residency Program until his 



 I have been an employee at BWH for 28 years. I will always remember completing the medical imaging bachelor’s degree program at Regis College thanks to the support of my department and tuition reimbursement, and then being promoted to clinical manager in Diagnostic Radiology.
I have been an employee at BWH for 28 years. I will always remember completing the medical imaging bachelor’s degree program at Regis College thanks to the support of my department and tuition reimbursement, and then being promoted to clinical manager in Diagnostic Radiology.
 I love taking part in our annual Pink Patch fundraiser. The goals of this Pink Patch fundraiser are to increase awareness about the importance of early detection and prevention and to raise funds to benefit the Comprehensive Breast Center at Brigham.
I love taking part in our annual Pink Patch fundraiser. The goals of this Pink Patch fundraiser are to increase awareness about the importance of early detection and prevention and to raise funds to benefit the Comprehensive Breast Center at Brigham.  Leah and I graduated PA school together and have both been at BWH for over 11 years, working together in OB-GYN. It was nice to actually hang out together outside of work with our other department PAs.
Leah and I graduated PA school together and have both been at BWH for over 11 years, working together in OB-GYN. It was nice to actually hang out together outside of work with our other department PAs.
 This summer, our Student Success Jobs Program (SSJP) interns worked as scribes for PACE, completed additional research hours and gained valuable pre-PA experience working as PCAs on our medicine units. Jessica McCarthy, PA-C, on PACE has been instrumental in creating this program, along with a few other PACE PAs, including Sarah Fittro, Alyssa Menard and Liz Ransom acting as mentors. We discovered this fall that our SSJP interns have been accepted into PA programs! Amazing work accomplished by all!
This summer, our Student Success Jobs Program (SSJP) interns worked as scribes for PACE, completed additional research hours and gained valuable pre-PA experience working as PCAs on our medicine units. Jessica McCarthy, PA-C, on PACE has been instrumental in creating this program, along with a few other PACE PAs, including Sarah Fittro, Alyssa Menard and Liz Ransom acting as mentors. We discovered this fall that our SSJP interns have been accepted into PA programs! Amazing work accomplished by all!









 Since last January,
Since last January, 








 When we look back on all that our Brigham community accomplished in 2023 to deliver high-quality and compassionate care, ignite discovery and innovation, educate the next generation of health care professionals and care for our communities, we are filled with a tremendous sense of pride in our incredible multidisciplinary teams.
When we look back on all that our Brigham community accomplished in 2023 to deliver high-quality and compassionate care, ignite discovery and innovation, educate the next generation of health care professionals and care for our communities, we are filled with a tremendous sense of pride in our incredible multidisciplinary teams.




 Brigham and Women’s Hospital mourns the loss of Lauren Alessandro, BSN, RN, of Braunwald Tower 12BC, Orthopaedics, who was known for the compassionate way she cared for both her patients and colleagues. She died unexpectedly on Oct. 15. She was 37 years old.
Brigham and Women’s Hospital mourns the loss of Lauren Alessandro, BSN, RN, of Braunwald Tower 12BC, Orthopaedics, who was known for the compassionate way she cared for both her patients and colleagues. She died unexpectedly on Oct. 15. She was 37 years old.



















 Brigham and Women’s Hospital mourns the loss of Woualid Wahnon, a supervisor in Environmental Services, who died Aug. 20 after a sudden illness. He was 45.
Brigham and Women’s Hospital mourns the loss of Woualid Wahnon, a supervisor in Environmental Services, who died Aug. 20 after a sudden illness. He was 45.

 Eligible patients are asked questions like “Do you have trouble paying your heating or electricity bill?” and “What is your housing situation today?” About half of patients screen “positive” for at least one SDoH question, meaning their response indicates they might be facing a nonmedical issue that could affect their health. Food access is the most common concern; nearly half of patients disclose that they run out of food before they have money to buy more. One in three patients say they have housing needs.
Eligible patients are asked questions like “Do you have trouble paying your heating or electricity bill?” and “What is your housing situation today?” About half of patients screen “positive” for at least one SDoH question, meaning their response indicates they might be facing a nonmedical issue that could affect their health. Food access is the most common concern; nearly half of patients disclose that they run out of food before they have money to buy more. One in three patients say they have housing needs.



 Hometown: Salt Lake City, Utah
Hometown: Salt Lake City, Utah Name: Richa Castellino, MBBS, MHA
Name: Richa Castellino, MBBS, MHA

